
What is a chalazion and how do you treat it? The many faces of chalazia.
Contributors: BCK Patel MD, FRCS, Jay Patel BSC, Raman Malhotra FRCS
Photographer: BCK Patel MD, FRCS
Posted December 19, 2021
Definition of a Chalazion: Traditionally, a chalazion is defined as the painless lump that develops on the eyelid, caused by the blockage of a Meibomian gland. These lumps enlarge slowly as the blocked Meibomian gland allows the lipogranulomatous material to expand within and eventually beyond the confines of the Meibomian gland. Initially, these lesions are rubbery and may become firm over time. Secondary inflammation or infection can make these lesions become tender to the touch. It is questionable if there is an inciting incidence of infection of the Meibomian glands leading to the formation of a chalazion.
When an area of inflammation is seen along the eyelid margin or within an eyelid, the terms stye, chalazion, internal hordeolum and external hordeolum are frequently used interchangeably. This is incorrect as each term describes a specific type of lesion and appearance.

Fig 1. A Chalazion with swelling of a Meibomian gland caused by retained lipogranulomatous material in a blocked Meibomian gland. Simple chalazia tend to be non-tender but will be firm to palpation

Fig 2. A Chalazion with erythema caused by secondary infection of the blocked Meibomian gland. These will be tender to the touch
Etymology: The Greek word “khalaza” means a “small knot”. The diminutive of “khalaza” is “khalazion”. Singular: “Chalazion”; Plural: “Chalazia” or “Chalazions”.
Synonyms: Tarsal cyst, Meibomian cyst, External hordeolum (see below), Internal hordeolum (see below)
Natural History: When a Meibomian gland opening becomes blocked, the sebaceous material within the gland expands causing a painless swelling, which is called a chalazion. They grow slowly and are initially painless. As the inflammation may spread to the surrounding tissues and secondary infection may occur, local tenderness may develop. Without intervention, chalazia may grow slowly over weeks to months and may become firm. They eventually resolve but can take weeks to months to resolve. When they become inflamed with or without infection and burst through to the external (skin) or internal (tarsal conjunctiva) surface, they resolve more promptly.
Chalazia are seen in childhood and also in adults in the 30 – 50 age group. Underlying conditions like acne rosacea and blepharitis can predispose to chalazia. Contrary to popular belief, use of contact lenses and use of makeup have not been associated with an increased incidence of chalazia. The wearing of masks during the Covid-19 pandemic has led to an increased incidence of chalazia, thought to be due to the drying effect of the flow of air behind the masks to the eyelid margins. A decrease in the use of masks has been shown to reduce the incidence of chalazia. A mechanical ptosis will occur with larger chalazia. Chalazia can also make it difficult to wear contact lenses because of the pressure of the enlarged glands on the cornea. In the lower eyelids, a mechanical ectropion may occur and can cause epiphora. Chronic chalazia may develop secondary calcification, which is seen in older patients. Development of malignancy with an initial formation of a chalazion is very rare.
External Hordeolum: Classically, the term “external hordeolum” is reserved for styes which are infections of the sebaceous oil glands (glands of Zeis) which open into the eyelash follicle. However, the term “external hordeolum” has also been used when a chalazion becomes infected and/or inflamed and erodes through the skin.

Fig 3. An inflamed or infected chalazion can point outwards. Although the term “external hordeolum” is usually reserved for infections of the glands of Zeis, this term is frequently also used for such an outward-pointing inflamed chalazion.

Fig 4. Another example of an inflamed chalazion pointing outwards where it sometimes breaks
Internal Hordeolum: When a Meibomian gland cyst (chalazion) becomes inflamed and points posteriorly to the tarsal conjunctiva or erodes through the tarsal conjunctiva, the lesion is often termed an “internal hordeolum”.

Fig 5. Internal hordeolum: the inflamed or infected Meibomian gland points posteriorly and a yellow surface is seen on the tarsal conjunctival surface where the lesion points.
Internal hordeola can cause local exuberant inflammation with a secondary pyogenic granuloma.

Fig 6. An internal hordeolum with a secondary conjunctival pyogenic granuloma
Meibomian Glands: Meibomian glands (also called tarsal glands) are glands within the tarsus of the upper eyelid and the lower eyelid. There are up to 30 such glands in the upper eyelid and 25 in the lower eyelid. They produce an oily substance called meibum which reduces the rate of evaporation of the tear film. They are exocrine glands, meaning they have ducts that secrete their contents via ducts that open at the eyelid margin. They are also holocrine glands because the secretions result from lysis of the secretory glands, thereby releasing the oily substance into the duct. Meibomian glands produce the oily substance called “meibum”, which forms the outer layer of the tear film and reduces evaporation of the aqueous component. Meibum also keeps the aqueous component from spilling over the edge of the eyelid by forming a film on the tear film and at the edge of the eyelid. Meibum also allows eyelids to shut into airtight closed units.
Etymology: Meibomian glands are named after Heinrich Meibom (1638 – 1700) who was a German physician who studied in France, Germany, Italy and England and went on to become a professor of medicine, and also a professor of history and poetry. Besides his medical treatises, he is also known for his Latin poetry.

Fig 7. Meibomian glands within the tarsal plates of the eyelids

Fig 8. Cross section of the upper eyelid showing the relationship of the Meibomian gland to the orbicularis oculi muscle and the eyelashes at the eyelid margin. The Meibomian glands open at the posterior part of the eyelid margin

Fig 9. Cross-section depiction of the eyelid margin showing the relationship of the Meibomian gland, the eyelashes and the glands of Zeis and Moll
Differential diagnosis of Chalazia:
Stye
Adenocarcinoma
Sebaceous gland carcinoma
Nodular basal cell carcinoma
Schwannoma
Histopathology of Chalazia: histopathology of a chalazion will reveal a lipogranulomatous reaction with multinucleated giant cells, neutrophils and lymphocytes with lipid vacuoles.
Management of Chalazia: It should be noted that a major review has shown that the traditionally accepted treatments for “internal hordeola” of warm compresses, over-the-counter topical medications, lid scrubs, prescribed antibiotics, steroids and eyelid massages have not been shown to be effective as non-surgical interventions. We present below what we have used successfully in our patients.
Acute Presentation: Most patients will present with a non-tender lump on an eyelid. The complaint is often one of cosmesis rather than discomfort or trouble with vision. However, a large chalazion can cause pressure on the cornea, creating astigmatism. Chalazia can also be in the line of sight when central.
Chalazia presenting early have lipogranulomatous material within the Meibomian gland. Traditionally, application of “warm soaks” four to five times a day, with or without the application of an antibiotic ointment or an antibiotic-steroid ointment is prescribed. Heat may be applied to the mass in any number of ways, including warm face-cloths, heated rice-pods, etc. The emphasis should be on pressure on the enlarged Meibomian gland. It is the pressure that allows the softening of the contents and possible egress of the material out through the “blocked” Meibomian gland orifice. Systemic antibiotics are rarely indicated for simple chalazia without evidence of cellulitis. Even when there is evidence of infection within the Meibomian gland, incision and curettage together with the application of topical antibiotic ointment will resolve the issue.
Chronic Chalazia: once chalazia have been present for several weeks, they become more firm. Although all chalazia will eventually resolve if left alone, patients are understandably keen to resolve them sooner. In such patients, incision and curettage is the best approach. This is usually performed via the conjunctival approach although, when the chalazion presents with an anterior break in the skin, it is reasonable to drain the chalazion through the anterior approach. When incising the mass from the tarsal surface, it is important to make the incisions vertically and not horizontally as some textbooks portray. There is no reason to make a crucifix incision and excise portions of the tarsus, as has also been promoted in ophthalmic textbooks. It is important to drain all the involved glands. Frequently, there will be more than one Meibomian gland involved. We use a specific technique to drain all glands that may be inspissated once the incision and curettage has been performed. This is demonstrated in the attached video.
Beware chronic chalazia and chalazia in older patients: sebaceous carcinoma can present with the appearance of a chalzion or multiple chalazia. The eyelid will have a yellowish appearance and the patient will not experience any discomfort. The slow growth with lack of pain and any associated loss of lashes should alert the physician to obtain a full-thickness biopsy of the eyelid and submit it fresh to the ophthalmic pathologist for appropriate staining, looking for evidence of sebaceous carcinoma.
Chronic chalazia with pyogenic granuloma: sometimes, with posterior perforation of a chalazion, a pendulous mass will present. There may be little material within the affected Meibomian gland.
Chalazia with cellulitis: in children, single or multiple chalazia can enlarge, become secondarily infected and cause a preseptal cellulitis. Indeed, whenever a child is seen with a cellulitis, the eyelids should be examined to palpate for any underlying chalazia. With appropriate treatment of the chalazia, the cellulitis will settle.
Intralesional steroid injection of chalazia: in early, soft chalazia, simple intralesional steroid injection will result in resolution of more than 50% of chalazia. With any chronic, firm or multiple chalazia, it is helpful to incise, drain and inject the surrounding tissues with intralesional steroids to enhance the resolution of the inflamed tissues with associated fibrosis.
Incision and Curettage: Patients who do not respond to topical ointments and warm soaks or where the lesions are chronic, large or multiple, incision and curettage is performed.
Instruments:
- Topical xylocaine drops or gel
- 11 Bard Parker blade
- 2% lidocaine with epinephrine on a 30 or 32 gauge needle
- Monopolar cautery
- Chalazion clamp
- Chalazion scoop
- Dexamethasone 4 mg/ml injection
- Gauze
- Eye patches
- Westcott scissors and 0.5 mm forceps may be needed
Surgical Steps:
- Soak the conjunctival surface with topical xylocaine drops or gel
- Evert the eyelid
- Apply the Gate theory (tapping, massage, rubbing of hands, arms, legs, etc) to reduce the perception of discomfort during the injection of local anesthetic
- Infiltrate the lesion with local anesthetic
- Apply the chalazion clamp and evert the eyelid
- Incise vertically over the affected Meibomian gland
- Curette the contents with a chalazion scoop
- Apply pressure to the treated and surrounded glands (see video) to ensure any other affected glands are also drained
- If there is a bleed, simple local cautery may be applied although this is rarely needed
- Some people apply carbolic acid to the cavity: we have not used this in our patients
- The eyelid will ooze for a few minutes: simple pressure will resolve this
- Application of ointment and a monocular occlusive dressing may be used
- When a chalazion is pointing anteriorly or has burst through the anterior surface of the eyelid, it is reasonable to perform curettage via the anterior of the eyelid
- Any granulomatous tissue is removed with sharp dissection
Chronic chalazion
A chronically blocked Meibomian gland can result in a firm nodule in the eyelid. By using the term “chronic chalazion”, the firmness and chronicity of such lesions can be recognized. These lesions require incision, curettage, injection with steroids and postoperative warm soaks. Resolution takes weeks. Also send tissue for histopathology if the lesion is showing no signs of resolution and has been recurrent or there are loss of lashes.

Fig 10. Chronic Meibomian gland cyst (chalazion) without local infection or inflammation resulting in a persistent, firm nodular lesion
The many faces of chalazia:

Fig 11. Combination of a chalazion and a stye affecting the right lateral lower eyelid. Patient also has a small inclusion cyst superomedially and a seborrheic keratosis on the lateral nasal wall. There are also multiple small papillomas

Fig 12. “Giant chalzion”: When a giant chalazion is seen, beware of other surrounding Meibomian glands being involved. These need incision and curettage

Fig 13. Early cellulitis of the lower lid from a chalazion. Such patients may need oral antibiotics besides incision and curettage and topical antibiotic ointment

Fig 14. A chalazion bursting through the eyelid skin with the appearance of a barley corn, therefore sometimes called an external hordeolum. These lesions can be drained anteriorly or posteriorly. When they heal, there is no risk of long lasting scarring
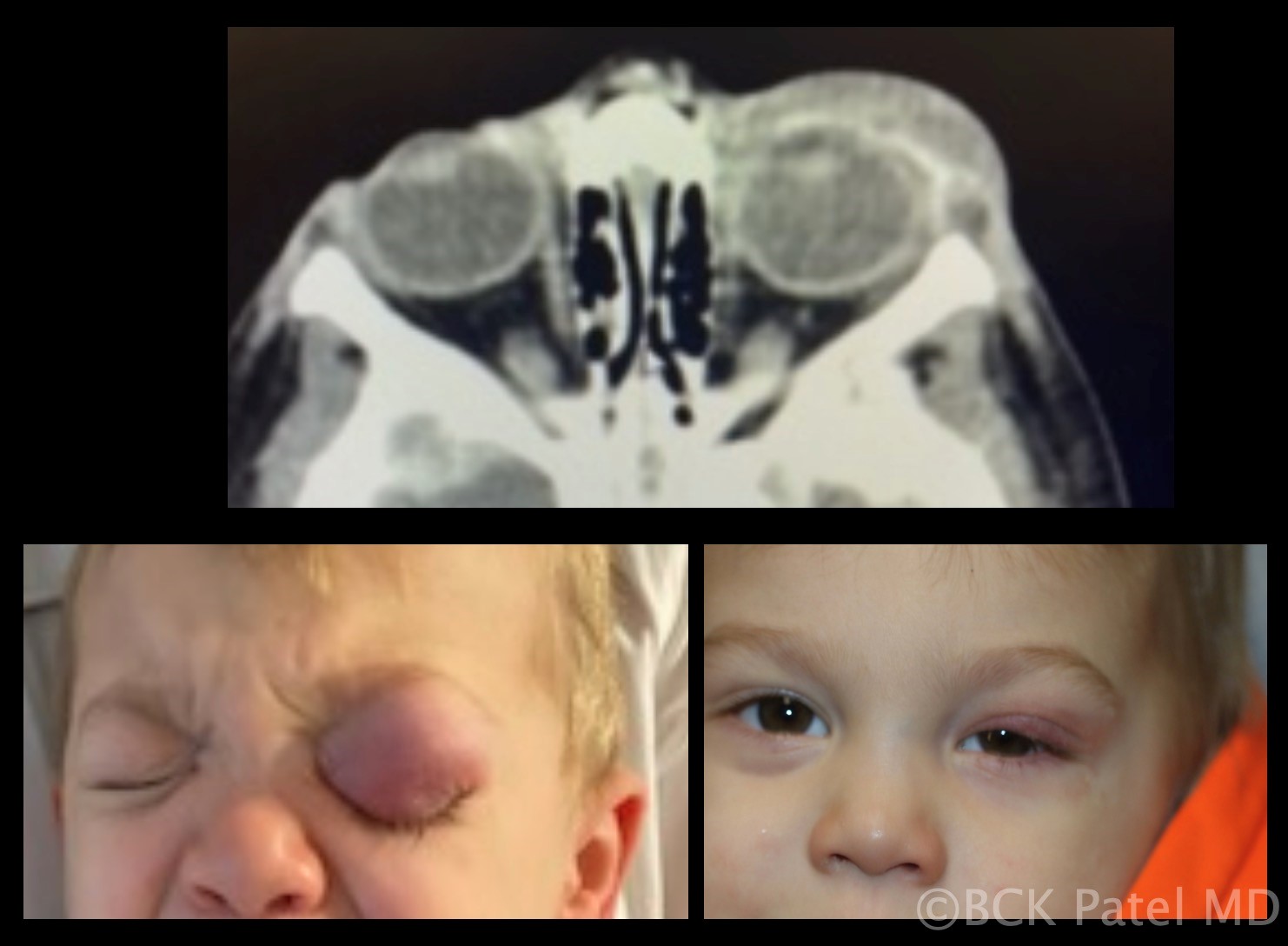
Fig 15. Underlying chalazia should be suspected with children present with preseptal cellulitis. In this child, there are several chalazia which are seen on the CT scan performed to ensure there were no postseptal changes. Treatment of the chalazia resolves the problem

Fig 16. A chalazion in a child presenting anteriorly. Once the lesion has burst through the surface as seen here, warm soaks and topical ointment will resolve this without need for surgical intervention

Fig 17. Chronic Meibomian gland cyst (chalazion) without local infection or inflammation resulting in a persistent, firm nodular lesion

Fig 18. Conjunctival granuloma without an obvious mass visible anteriorly. These are chalazia that erode through the tarsal conjunctival surface with local secondary inflammation. The granuloma needs to be excised in addition to incision and curettage of the chalazion and injection with steroid

Fig 19. An example of a left lower eyelid chalazion which was treated with warm soaks and topical ointment. The photograph below was taken one month later showing complete resolution of the chalazion
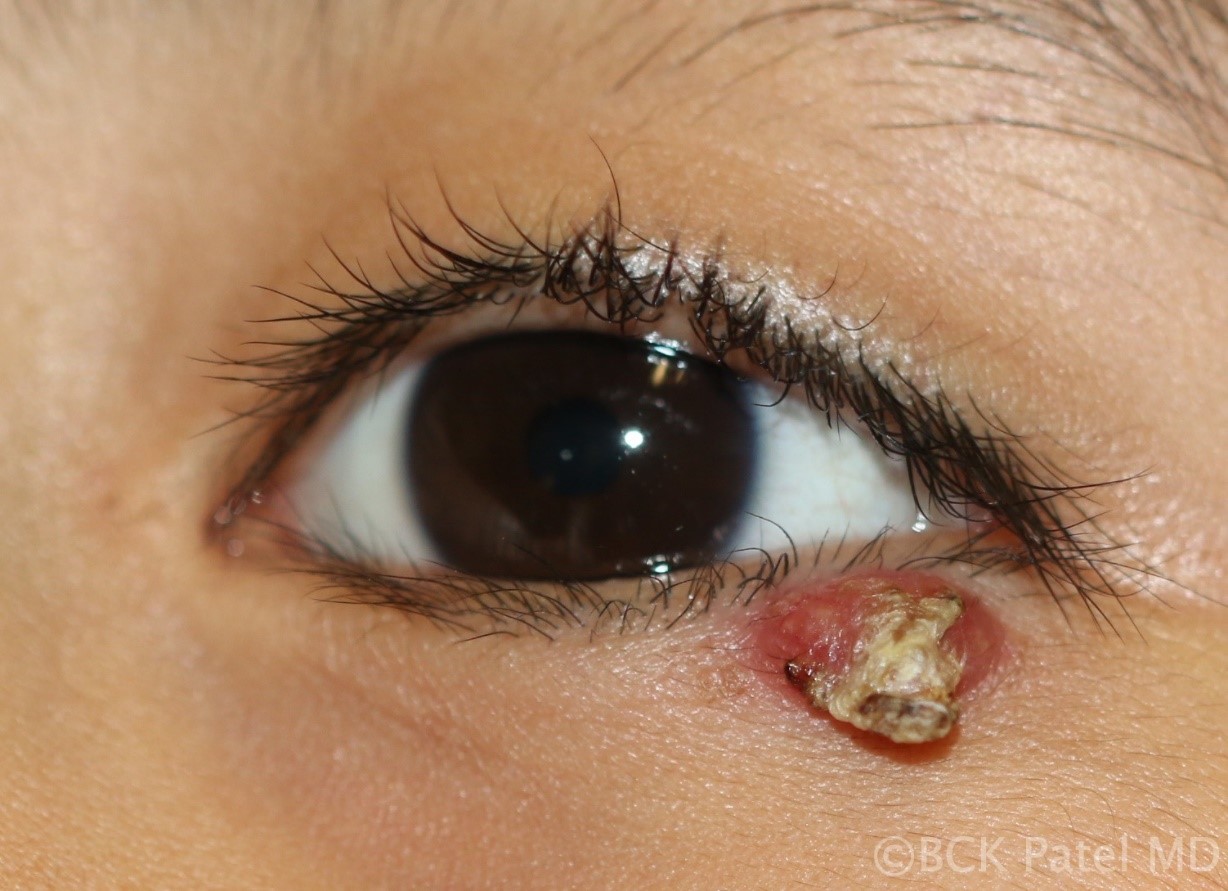
Fig 20. Chronic chalazion which has burst through to the surface. These will respond to topical warm soaks and topical ointment

Fig 21. Resolving Chalazion: Once the lesion starts to resolve, wrinkling of the eyelid skin over the lesion will be seen with decreasing swelling. These will resolve with conservative management

Fig 22. Inflamed chalazion in a child pointing anteriorly. With warm soaks, these will burst through the skin and eventually resolve with conservative treatment
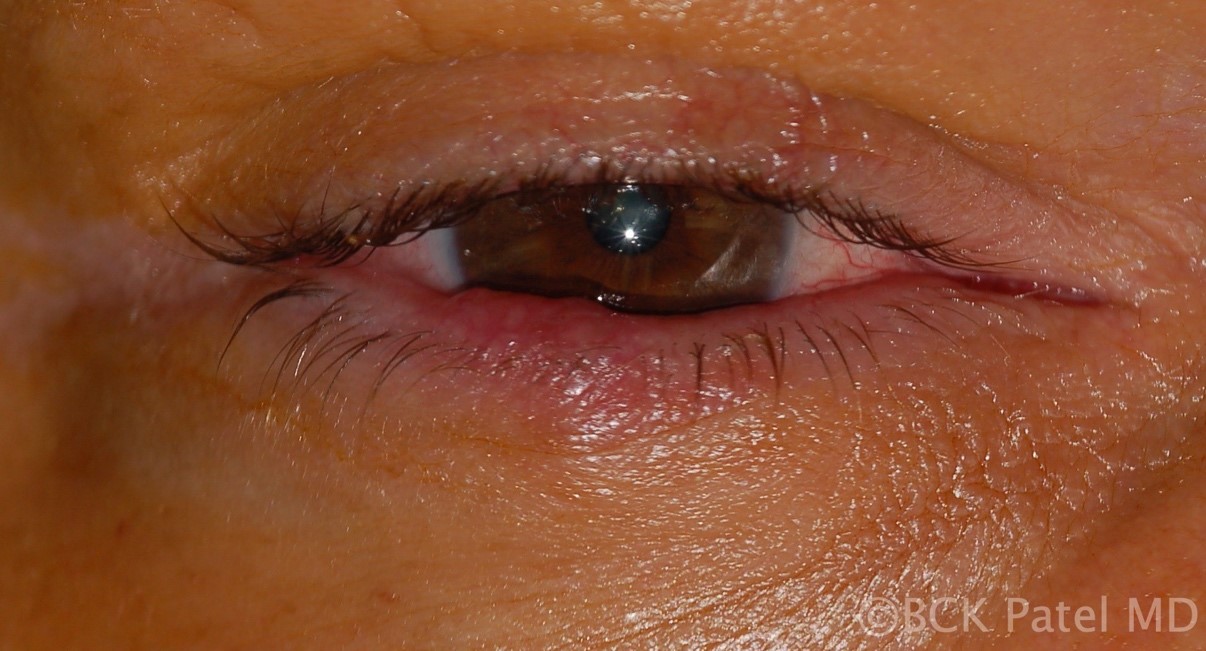
Fig 23. Chronic meibomianitis in a patient with chronic Meibomian gland disease with recurrent chalazia. These patients will need oral tetracycline together with management of any associated acne rosacea in addition to lid margin management. There can be reduction in eyelashes even in the absence of malignancy in these patients but if in doubt, a biopsy should be performed

Fig 24. Chronic chalazion which “has been present for six months”. There is no tenderness but the mass is visible. These patients will need incision and curettage with injection of steroids. The firm lining of the chronic chalazion will take weeks to soften and resolve

Fig 25. Multiple chronic chalazia affecting the upper and lower eyelids. In older patients, a biopsy should be obtained in such patients

Fig 26. Multiple chalazia eroding through the eyelid skin. These will need incision and curettage through the anterior approach and steroid injection. The surrounding Meibomian glands should also be expressed in these patients.

Fig 27. A typical “External Hordeolum”, or chalazion presenting anteriorly. These will need incision and drainage anteriorly

Fig 28. A firm hard nodule of six-months-duration: chronic chalazion. This will not respond to simple intralesional steroid injection but will need incision and curettage as well as steroid injection, warm soaks and topical ointment

Fig 29. Sessile conjunctival granuloma associated with a chalazion: these need resection of the granuloma, incision and curettage of the chalazion and injection with steroid

Fig 30. Medial upper eyelid chalazion: a Q-tip can be used to show the point where the gland is enlarged, thereby making incision easier

Fig 31. A giant chalazion. This started as a single chalazion but the inflammation has spread along the eyelid and other Meibomian glands are now also involved. In such patients, it is important to palpate and identify all the glands involved so they may be incised and drained properly

Fig 32. An example of an “external hordeolum” resembling a corn of barley. Note that the area of inflammation is not just at the root of a lash, as would be the case with a stye

Fig 33. Large chalazion in a child. These children will often have other smaller chalazia so when performing an incision and curettage, it is best to examine all four eyelids

Fig 34. Internal hordeolum type of chalazion

Fig 35. Chronic chalazion close to the upper punctum. When performing procedures on these, it is important to protect the punctum and canaliculus

Fig 36. This is how typical chalazia will present with redness and some swelling on the conjunctival side

Fig 37. Chalazion presenting with posterior presentation. These do well with incision and curettage

Fig 38. Example of multiple chronic chalazia affecting all four eyelids. Contrary to popular belief, there is no evidence that diet has any effect on chalazia. Many such patients will also have no evidence of acne rosacea or blepharitis or meibomianitis

Fig 39. Chronic Meibomian gland cyst (chalazion) showing the involvement of several adjoining Meibomian glands next to the lower punctum
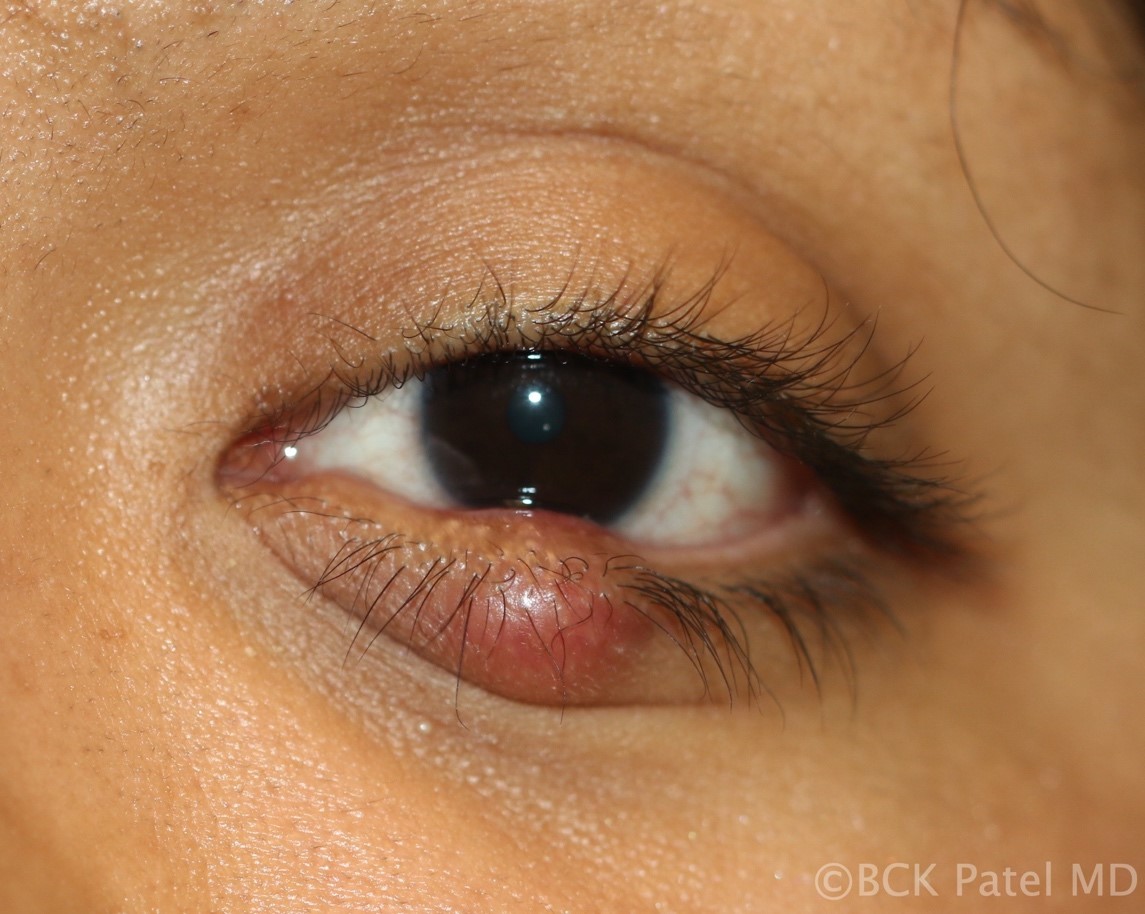
Fig 40. A firm chronic chalazion with distortion of the eyelashes but no loss of eyelashes. These will take time to resolve even after incision, curettage and steroid injection

Fig 41. Resolving chalazion: this is a typical example of when nothing active needs to be done other than warm soaks. The chalazion is resolving with the “wrinkling” of the skin over the lesion and shrinkage of the lesion

Fig 42. An acutely inflamed external hordeolum (chalazion). These are best drained externally

Fig 43. Children will often be brought with this appearance with the claim that “the bumps have not gone away”. Chronic chalazia can take weeks to months to resolve. Topical steroids may be prescribed for a short course to expedite the resolution. The parents should be reassured that the “bumps” will go away and there will be no residual scarring left. It can be difficult to convince parents of this, however!

Fig 44. Multiple chronic chalazia in a child. Young children often get multiple chalazia affecting more than one eyelid. No specific cause of this has been identified and there is no defined way of preventing this. When chronic, these will need incision and curettage under general anesthesia. All four eyelids should have the Meibomian glands expressed during the procedure. Furthermore, it should be explained to the parents that there is no way of ensuring that other Meibomian glands do not become blocked or inflames some days, weeks or months later!

Fig 45. Chalazion in skin of color. Steroid injection can lead to hypopigmentation and should be used judiciously. Otherwise, the management is the same as for other chalazia
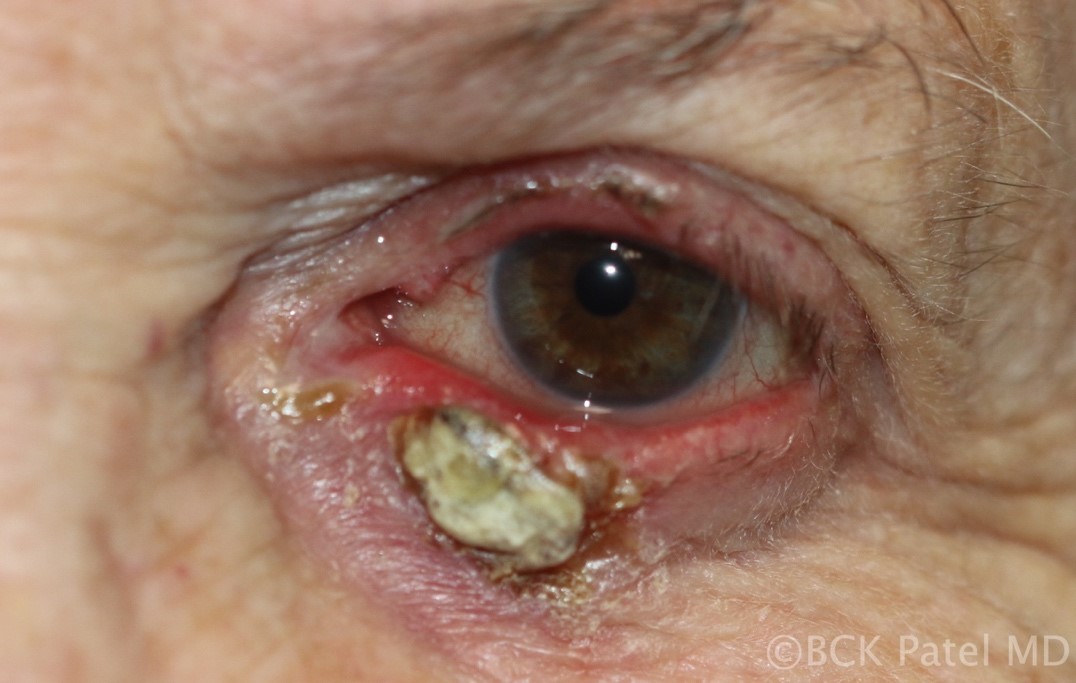
Fig 46. Chronic chalazion with anterior ulceration and calcification. In such lesions, it is important to send samples for histopathology to exclude underlying malignancy

Fig 47. Acute chalazion with spread of infection into the subcutaneous tissue leading to early preseptal cellulitis.
References
- Jordan GA, Beier K. Chalazion. StatPearls, Treasure Island (FL): StatPearls Publishing. Aug 2021. https://pubmed.ncbi.nlm.nih.gov/29763064/ PMID:29763064
- WillmannD, Guier CP, Patel BCK,, Melanson SW. Stye. StatPearls, Treasure Island (FL): StatPearls Publishing. Aug 2021. https://pubmed.ncbi.nlm.nih.gov/29083787/ PMID:29083787
- Lindsley K, Nichols JJ, Dickersin K. Non-surgical interventions for acute internal hordeolum. Cochrane Database Syst Rev 2017 Jan 9;1(1):CD007742 PMID:28068454